The pituitary is a small gland located below the brain in the skull base, in an area called the sella tursica. The pituitary gland is often called the master gland because it controls the secretion of all the major endocrine hormones. These compounds have broad ranging effects on metabolism, fluid control, growth, and sexuality.
The pituitary gland is divided into a larger anterior region (adenohypophysis) and a smaller posterior region (neurohypophysis). The gland is connected by the pituitary stalk to the hypothalamus, located directly above the pituitary gland. Because of the close proximity of the pituitary gland to the major intracranial nerves and blood vessels and its overall control of the endocrine systems, pathologies of the pituitary can cause a wide spectrum of symptoms, both hormonal and neurological.
Pituitary Hormones
Thyroid Stimulating Hormone (TSH)
TSH stimulates the thyroid gland to release thyroid hormones (T2, T3, T4). Thyroid hormones affect almost all cells of the body, controlling basal metabolic rate and playing a crucial role in growth. Excess TSH is the cause of secondary hyperthyroidism. TSH deficiency causes secondary hypothyroidism, which can result in short height with short extremities.
Growth Hormone (GH)
This hormone is a peptide produced and secreted by the anterior pituitary gland. GH is stimulated by growth hormone-releasing hormone (GHRH) and is inhibited by somatostatin. The pituitary produces more GH than any other hormone. GH does not exert all its effect directly. Many of its effects are caused by insulin-like growth factor (I-GH), also known as somatomedin-C.1
GH is the principal hormone regulating growth. It stimulates not only muscle and bone growth, but also the growth of internal organs. It has anabolic activity, stimulating bone and muscle growth in childhood. GH also functions to raise blood sugar levels by gluconeogenesis and works as an antagonist of insulin.
GH naturally decreases by 14% per decade after age 20. When the hormone is secreted in excess, it causes gigantism (acromegaly). Excessive GH replacement therapy has been shown to cause cardiac hypertrophy, carpal tunnel syndrome, diabetes, and musculoskeletal tissue disorders.
Deficiency causes dwarfism when it occurs during growth. In adults, GH deficiency is also linked to decreased life expectancy, cardiovascular disease, and bone loss. Deficiency is caused by chronic stress, cortisol, progesterone, serotonin antagonists, obesity, hyperthyroidism, and hyperglycemia.
Adrenocorticotropic Hormone (ACTH)
ACTH triggers the adrenal cortex to release glucocorticoid steroids (cortisol and cortisone) and mineralocorticoids (11-Deoxycortiocsterone and aldosterone). ACTH deficiency causes secondary hypoadrenocorticism (Addison’s disease). ACTH excess causes hyperadrenocorticism (Cushing’s disease).
Leuteinizing Hormone (LH) and Follicle-Stimulating Hormone (FSH)
These hormones control reproduction. LH promotes ovulation and progesterone production in females and testosterone production in males. FSH promotes ovum formation and estrogen production in females and spermatozoa formation in males.
In females, a deficiency of LH is associated with PMS, while a deficiency of FSH is associated with PCOS. A deficiency of both LH and FSH is the cause of amenorrhea of pituitary origin. Conversely, excess LH is seen in PCOS, while excess FSH contributes to PMS. The most common cause of a combined excess of LH and FSH is menopause. In males, LH deficiency causes hypogonadism, while FSH deficiency is associated with infertility.
Prolactin (PRL)
This hormone stimulates secretion of breast milk by stimulating the mammary glands. It also suppresses ovulation and stimulates the thymus gland.
Excess prolactin is associated with a high estrogen/ progesterone ratio, infertility, galactorrhea, and polycystic ovary syndrome (PCOS). Insufficient prolactin is associated with deficient lactation.
Anti-Diuretic Hormone (ADH)
Also known as vasopressin, this hormone promotes water retention by increasing the kidney’s reabsorption of sodium at the distal renal tubules. ADH promotes the production of concentrated urine.
A deficiency of ADH causes diabetes insipidus. Excess ADH causes hypervolemia and hypertension.
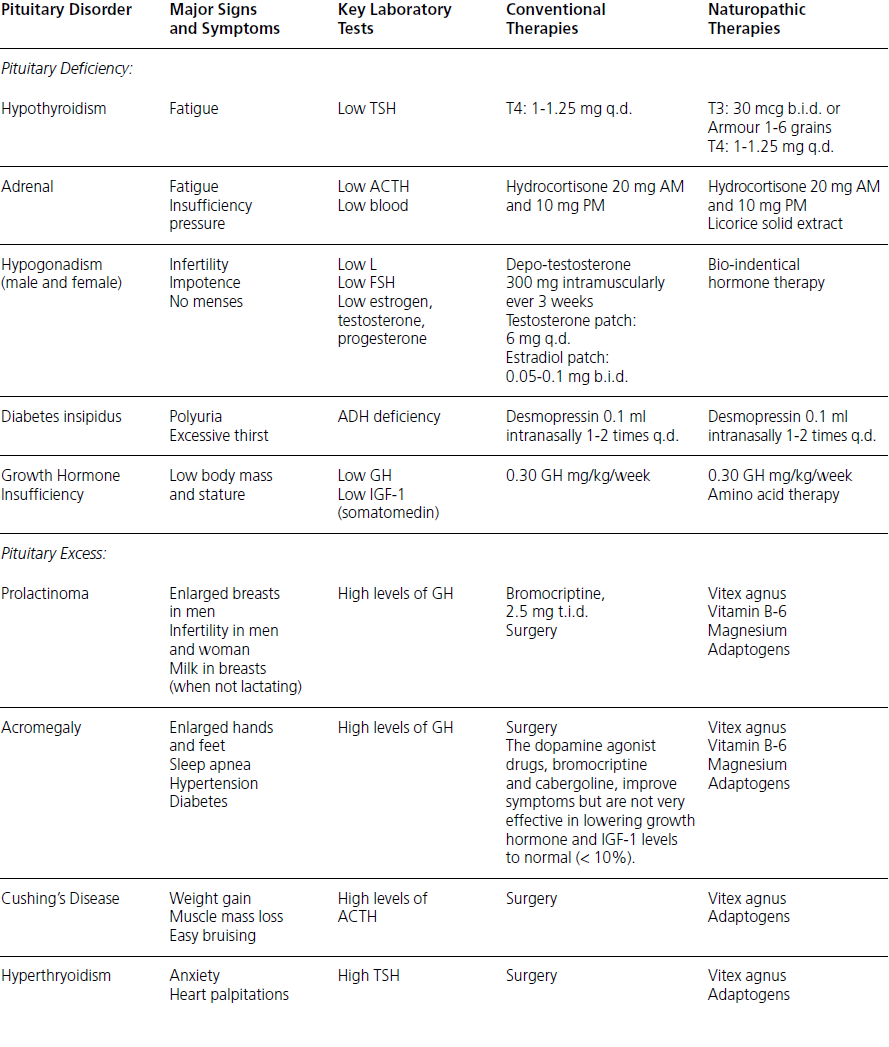
Quick Reference: Pituitary Disorders
Note: Many naturopathic therapies for hormone deficiency are similar to conventional therapies. In cases of pituitary excess, specific naturopathic approaches would use dosing of Vitex agnus castus (chasteberry) from 20-200 mg t.i.d. and adaptogenic herbs 500 mg – 3 grams t.i.d. However, in severe cases surgery might still be needed.
Hypopituitarism (Pituitary Insufficiency)
Pituitary insufficiency is defined as failure of the gland to make one or more of the following anterior pituitary hormones: growth hormones (GH), prolactin (PRL), adrenocorticotropin (ACTH), thyrotropin (TSH), leuteinizing hormone (LH), or follicle-stimulating hormone (FSH).
Hypopituitarism can be caused by factors that disrupt normal pituitary function. These include pituitary, hypothalamic, or parasellar disease, which causes displacement, infiltration, or destruction of the gland. Examples include meningiomas, craniopharyngiomas, optic nerve gliomas, nasopharyngeal tumors, and pineal dysgerminomas.
If damage is located at the pituitary stalk, all the anterior pituitary hormones (TSH, LH, FSH, GH, and ACTH) decrease, while prolactin (PRL) rises. This rise in prolactin results from the loss of the inhibitory effect of hypothalamic dopamine on the lactotrophs.
Signs and Symptoms
Non-specific symptoms, such as fatigue and weight loss (and other symptoms of adrenocortical insufficiency), are often due to ACTH deficiency. Physical characteristics, such as pubic and axially hair loss in women, with serum sodium levels being low, are also indicative of low ACTH release by the pituitary. Morning cortisol values lower than 10 ug/dl or ACTH stimulated values less than 20 ug/dl are considered indicative of secondary adrenal insufficiency.
Hypothyroidism is primary when the thyroid is not working, as in thyroiditis or Hashimoto’s disease. However, in secondary hypothyroidism, thyroid hormone deficiency is secondary to loss of hormones secreted by the pituitary of hypothalamus. The signs and symptoms of secondary hypothyroidism are usually milder than primary hypothyroidism. In some cases, massive pituitary tumors may not result in obvious signs of hypothyroidism. TSH ranges may be only mildly lowered, with T3 in the normal range and with normal to low T4 levels.
The single most important hormone deficiency to identify is cortisol because cortisol deficiency can be life threatening.
Conventional Medical Treatment
This would include the use of growth hormone injection. It has been successfully done for the last 30 years. Currently, growth hormone therapy is available from recombinant DNA therapy rather than human cadavers. The injections are administered subcutaneously with a weekly dose totaling 30 mg/kg per week.
Naturopathic Medical Treatment and Prevention
In addition to standard growth hormone injections, amino acid therapy is recommended to help stimulate human growth hormone level. The use of arginine intravenously has demonstrated to be effective in increasing growth hormone levels. Orally 5 g and 9 g of arginine caused a significant GH response. However, at higher doses, such as 13 g, digestive side effects occurred with no further increase of GH stimulation. The rise in GH concentration occurs within 30 minutes and peaks at 60 minutes after oral ingestion.6
Hyperpituitarism (Pituitary Excess)
Cushing's Syndrome and Disease
The normal function of cortisol in healthy subjects is to increase glucose production, inhibit protein synthesis, increase lipolysis, increase protein breakdown, and modulate immunological and inflammatory responses. ACTH is stimulated by corticotropin-releasinghormone (CRH). Cortisol suppresses the release of ACTH and CRH. Because of the wide variability of cortisol secretions in a 24-hour period, frequent saliva hormone testing during the course of a day can be helpful rather than a single blood draw to measure cortisol levels.
Cushing’s syndrome is a non-specific name for excessive serum glucorticoids. The two main causes include exogenous glucorticoid ingestion (e.g., patients taking steroid medications, typically for inflammatory states) and pituitary dysfunction, which causes a condition that is known as Cushing’s disease.
Cushing’s disease is caused by excess ACTH in 80% of cases. Of these ACTH dependent cases of Cushing’s, 85% are caused by a pituitary disorder (typically a benign adenoma) that affects ACTH production. The remaining 15% are caused by ectopic ACTH producing tumors, such as malignant tumors of the lungs.
Conventional Medical Treatment
Surgery is often recommended if Cushing’s disease is caused by benign adenoma of the pituitary.
Naturopathic Medical Treatment and Prevention
Specific therapy for benign adenoma is the use of Vitex agnus and adaptogenic herbs. Clinical studies have only been done on horses, although it has been used successfully in human clinical practice as well. The successful treatment of equine Cushing’s syndrome in decreasing pituitary adenoma is one of the best examples of treating a disease using a naturopathic approach.7
Pituitary Tumors
Pituitary tumors usually make two or more hormones at the same time. In some cases, significant hormones are produced than can end up causing characteristics of several endocrine pathologies simultaneously. Symptoms depend on the type and location of the tumor and whether the tumor causes hormone excess, hormone deficiency, or pressure on the brain and central nervous system. Thus, one type of pituitary tumor may produce symptoms that are very different from those produced by another type of growth. In addition, some tumors may begin by causing the release of excess hormone and then later result ina hormonal deficiency as normal pituitary cells are suppressed, thereby confounding a proper diagnosis.
Gonadotropinoma
Gonadotropinomas secrete the glycoproteins LH and/or FHS, which may lead to an excess of these hormones. Although they do not always cause endocrine disturbances, these tumors usually cause neurological problems because of their size.
Thyrotropinoma
Whenever patients have high levels of T3 and T4 and a detectable TSH level, a TSH-secreting tumor should be suspected. The conventional treatment includes pituitary ablation. Bromocriptine, a drug that is used to suppress TSH secretion, is usually not that effective.
Not all patients with pituitary tumors and elevated TSH have thyrotropinomas. Patients with long-term untreated hypothyroidism can cause a pseudo tumor as a compensation for the pituitary producing high levels of TSH for the low function of the thyroid gland. For this reason, no patients should go under surgical intervention of pituitary masses without first checking the TSH and T4 levels simultaneously.
Signs and symptoms of thyrotropin adenomas include weight loss, increased appetite, heart palpitations or irregular heartbeat (superventricular tachycardia, atrial fibrillation), tachycardia (rapid heart rate), heat intolerance and increased sweating, tremor, frequent bowel movements, fatigue and muscle weakness, exertional intolerance and shortness of breath, oligomenorrhea (decreased menstrual flow), nervousness and irritability, other mental disturbances, sleep disturbances (including insomnia), changes in vision, photophobia, eye irritation, diplopia or exophthalmos, lower extremity edema (swelling), sudden paralysis, and impaired fertility.
HyperProlactinemia
Hyperprolactinemia is a common disorder characterized by excess PRL production by the anterior pituitary. Causes of elevated levels of serum prolactin are pituitary tumors, such as pituitary adenoma. Other causes include interferences with the hyopthalamic pituitary pathway, such as caused by tumors, trauma, or surgery, as well as pharmacological agents that interfere with dopaminergic input to the pituitary gland cause elevated prolactin. These drugs are Phenothiazines, Tricyclic antidepressants, Apha-Methyldopa, Metoclopramide, Cimetidine, and estrogens. In prolactin-secreting pituitary adenomas, monoclonal cell populations autonomously produce prolactin. Generally, the most important physiological states in which prolactin is found to be elevated in healthy adults are pregnancy and lactation.
Symptoms and Signs
Symptoms include anxiety, depression, irritability, and weight gain. In women, since excess PRL causes an increase in the estrogen/progesterone ratio, menstrual cycle irregularities, amenorrhea, anovulation, infertility, and ovarian cysts (PCOS) are possible. Hyperandrogenism and insulin resistance are also symptoms of elevated progesterone/estrogen ratio. In men, excess PRL is associated with low libido and erectile dysfunction.
Functional hyperprolactinemia can also be assessed by measuring basal body temperature charting. This charting would show an absence of increased body temperature indicating anovulation because, during ovulation, body temperature normally increases.8
Conventional Medical Treatment
The dopamine agonist, bromocriptine mesylate, is the initial drug of choice for treating hyperprolactinemia. It lowers the prolactin level in 70% to 100% of patients. However, side effects are common and may include drowsiness, digestive disturbances, headache, and insomnia.
Radiation treatment is another option; however, its benefits in routine treatment have not been shown to outweigh the risks. Radiation is, therefore, typically reserved for rapidly growing tumors.
Surgical care is indicated in patient drug intolerance, tumors resistant to medical therapy, patients who have persistent visual-field defects in spite of treatment, and patients with large cystic or hemorrhagic tumors.
Naturopathic Medical Treatment and Prevention
Bio-identical Hormones and Clinical Nutrition
Naturopathic treatment of hyperprolactinemia includes the use of nutrients (such as vitamin B-6 and magnesium) that promote dopamine synthesis, since dopamine is the main inhibitor of prolactin. If an elevated estrogen/progesterone ratio is detected, this can be treated with nutrients that promote estrogen metabolism, and/or with bio-identical progesterone replacement.
Dopamine is the key modulator of prolactin and acts as an inhibiting factor. Progesterone also is used because it opposes PRL-induced excess estrogen.
Botanical Medicine
Botanicals that are known to inhibit PRL, such as chasteberry (Vitex agnus castus), are indicated. Animal studies confirmed that vitex agnus works comparatively as well as dopamine agonists, such as lisuride, by significantly inhibiting TRH-stimulated prolactin secretion of rat pituitary cells. Because of its dopaminergic effect, vitex can be considered an efficient alternative to drugs in slight hyperprolactinemia.9
Vitex at a dose of 20 mg vs placebo was administered to 52 women with luteal phase defects due to latent hyperprolactinemia. The treatment group had a statistically significant reduction in prolactin, luteal phase was normalized, and progesterone levels normalized. Two women got pregnant during the study while taking vitex. No side effects in the study were noted.10
Lifestyle
Stress management, aerobic exercise in moderation, and avoidance of hypoglycemic episodes are also indicated.
Powell D. Endocrinology and Naturopathic Therapies. Seattle, WA, Bastyr University, 2004.
Svensson J, Mattsson A, Rosen T, Wiren L, Johannsson G, Bengtsson BA, Koltowska Haggstrom M. Swedish KIMS National Board. Three-years of growth hormone (GH) replacement therapy in GH-deficient adults: Effects on quality of life, patient-reported outcomes and healthcare consumption. Growth Horm IGF Res. 2004 Jun;14(3):207-15.
Rudman D, Feller AG, Nagraj HS et al. Effects of human growth hormone in men over 60 years old. New Eng. J. of Med 1990;323:1-6.
Ehrnborg C, Ellegard L, Bosaeus I, Bengtsson BA, Rosen T. Supraphysiological growth hormone: Less fat, more extracellular fluid but uncertain effects on muscles in healthy, active young adults. Clin Endocrinol (Oxf). 2005 Apr;62(4):449-57.
Collier SR, Casey DP, Kanaley JA. Growth hormone responses to varying doses of oral arginine. Growth Horm IGF Res. 2005 Apr;15(2):136-39. Epub 2005 Jan 26.
Harmany Equine Clinic, Ltd, Washington, Virginia 22747, USA. The role of nutritional therapy in the treatment of equine Cushing’s syndrome and laminitis. Altern Med Rev. 2001 Sep;6 Suppl:S4-16.
Powell D. Endocrinology and Naturopathic Therapies. Seattle, WA: Bastyr University, 2004.
Sliutz G, Speiser P, Schultz AM, Spona J, Zeillinger R. Agnus castus extracts inhibit prolactin secretion of rat pituitary cells. Horm Metab Res. 1993 May;25(5):253-55.
Milewicz A, Gejdel E, Sworen H, Sienkiewicz K, Jedrzejak J, Teucher T, Schmitz H. Vitex agnus castus extract in the treatment of luteal phase defects due to latent hyperprolactinemia. Results of a randomized placebo-controlled double-blind study. Arzneimittelforschung 1993 Jul;43(7):752-56.
This website uses cookies to improve your experience. We assume you are ok with this, but you can opt-out if you wish.
Read More
Cookies are small text files that can be used by websites to make a user's experience more efficient. The law states that we can store cookies on your device if they are strictly necessary for the operation of this site. For all other types of cookies we need your permission. This site uses different types of cookies. Some cookies are placed by third party services that appear on our pages.
For more information on how Google's third party cookies operate and handle your data, see:
Google's Privacy Policy
Necessary cookies help make a website usable by enabling basic functions like page navigation and access to secure areas of the website. The website cannot function properly without these cookies.
Marketing cookies are used to track visitors across websites. The intention is to display ads that are relevant and engaging for the individual user and thereby more valuable for publishers and third party advertisers.
Preference cookies enable a website to remember information that changes the way the website behaves or looks, like your preferred language or the region that you are in.