Abstract
Background: Shamanism is a transcultural, heterogeneous worldview that is primarily concerned with human interaction with the spirit world. Foremost among the many services provided by practitioners of shamanism is the healing of the mind, body, and spirit.
Methods: While most literature on shamanism consists of ethnographies of cultures that practice shamanism, the present literature search was performed to review existing medical literature of shamanic healing as a clinical intervention.
Results: Sixteen publications met the inclusion criteria, encompassing 1 clinical trial, 2 case series, and 10 case reports.
Conclusions: Our findings demonstrate that shamanic healing as an intervention has potential benefits and a relatively low risk of harm, and is feasible to investigate as a clinical intervention. Further research is warranted to better elucidate its benefits.
Introduction
Shamanism is a non-dogmatic spiritual worldview that is not a religion, is found across cultures, and includes shamans or shamanic practitioners who use altered states of consciousness (ASC) to perform services.1,2 Foremost among those services is the healing of the body, mind, and spirit.3 The term shaman was first introduced to the Western world by Mircea Eliade (1907–1986), professor of the history of religion. He borrowed the term from the Tungusic people of Siberia and Central Asia, but he suggested in his work on the subject Shamanism: Archaic Techniques in Ecstasy4 that the term could be applied across cultures for those fulfilling a similar role with similar practices.
Michael Harner (1929–2018), an anthropologist, after spending several years in the Peruvian Amazon with indigenous groups, founded the Center for Shamanic Studies in 1979 in an effort to focus on common threads of shamanism throughout the world. A year later, he published The Way of the Shaman,5 the foremost guide on the subject for practitioners, which in addition to his training workshops and other efforts made him and his methods central in the neo-shamanic movement.6 It has been said of him, “what Yogananda did for Hinduism and D. T. Suzuki did for Zen, Michael Harner has done for shamanism, namely bringing the tradition and its richness to Western awareness.”7
Though there are many heterogeneous shamanic practices across cultures, including divination for the purpose of hunting, spiritual, as well as literal warfare, and more,8 Harner describes and teaches what he has called core shamanism, which consists of the common elements found across cultures, with the cultural elements removed, and the practices adapted for a Western audience. In this shamanic paradigm, the health of the mind, body, and spirit is inseparable from the community, nature, and cosmos, while illness has both physical and non-physical or spiritual causes.5 Shamanic healing practices primarily deal with the spiritual elements that lead to illness and can be broadly categorized as either soul loss, the loss of spiritual energy that is vital to one’s well-being, or the intrusion of detrimental spiritual energies.
Central to the practice of shamanism is the use of ASC. In some cultures, the initiation of a shaman can only be considered if that individual has manifested and/or has a family history of what Westerners would consider mental illnesses, such as schizophrenia or bipolar disorder, that feature hallucinations.8 Despite Westerners’ pathologizing and misunderstandings of such cultural practices, their perspective is not ubiquitous. Techniques of inducing altered states also include fasting, dancing, psychedelic plants, and meditation.9 Western practitioners of core (neo-)shamanism typically use drumming or rattling (sonic driving) in the range of 4–7 Hz to induce ASC. In his original work, Neher investigated how the sonic driving of the drum entrained the human cerebral cortex into a sinusoidal waveform.10,11
A recent electroencephalography (EEG) study showed that sonic driving increased gamma power, which correlated with visual alterations and increased criticality in the low beta band, correlating with complex imagery and elementary visual alterations. However, the EEG signature of the shamanic trance was distinct from psychedelic drug-induced states and displayed unique traits.12 During shamanic trance (ASC), practitioners often ask for guidance and support from spiritual entities, such as power animals and ancestors, for the purpose of performing healing that may involve soul retrievals, power animal retrievals, extractions, or other techniques on behalf of the client they are attempting to help.5,13–15
Despite evidence and demand for spirituality in the delivery of healthcare,16,17 doing so remains taboo. This is especially true in the case of shamanic healing as a clinical intervention, for which there has been very little clinical research, despite a robust literature in the fields of anthropology and religion. The intention of the present study is to collate available clinical data on shamanic healing practices as a primary intervention.
Methods
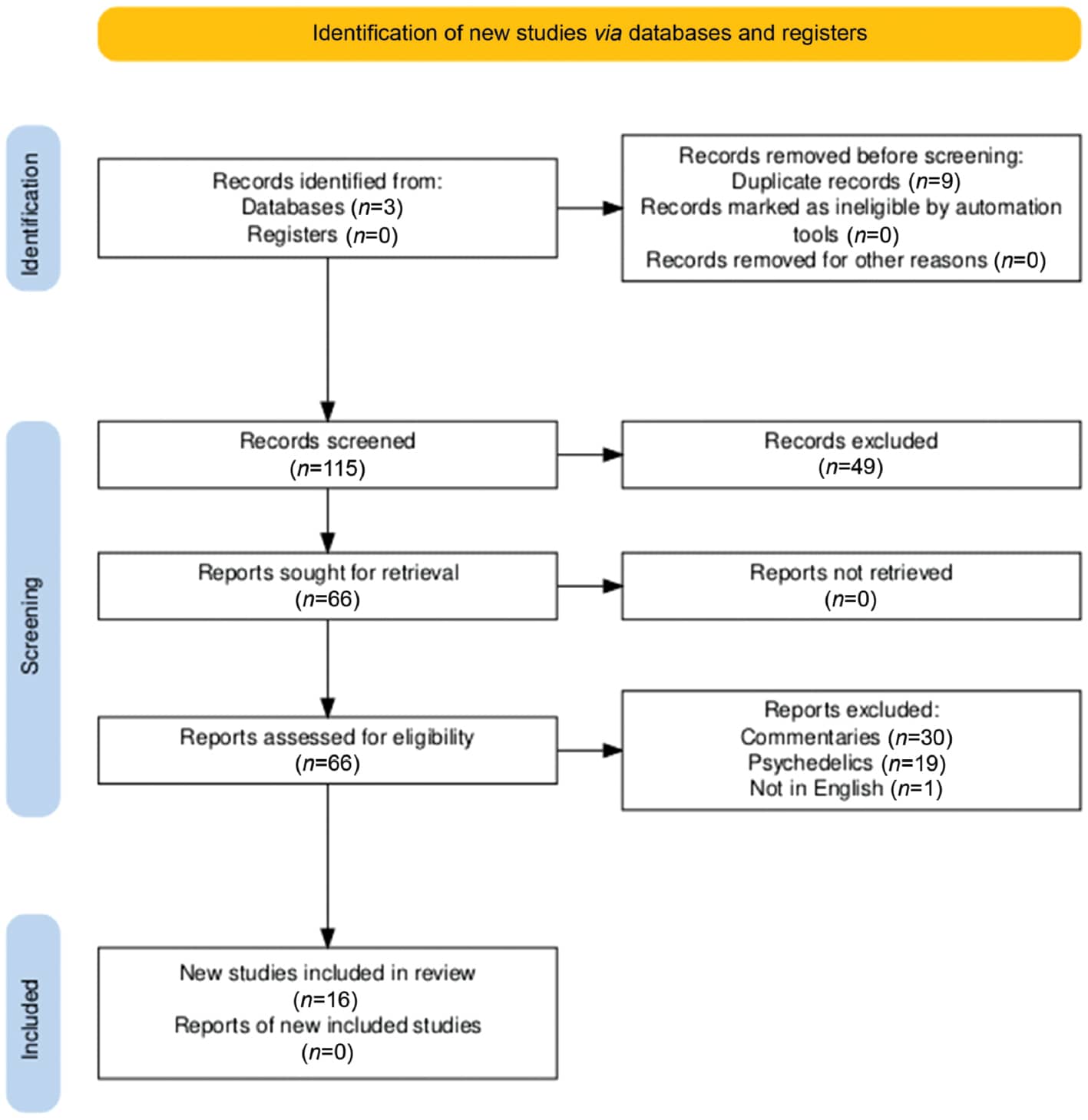
We conducted a literature search using PubMed, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Scopus with the following search terms: ““shaman*” AND (case report OR case series OR clinical trial)”. The use of an asterisk (*) at the end of the word gave us results with all possible endings including “shamanism,” “shamanic,” etc. The search was conducted on January 9, 2024, and updated on August 25, 2025. While shamanic practices are intimately related with psychedelic plant medicines in many cultures,2 we decided to exclude studies that involved pharmacological interventions in order to keep our research focused. We included three case reports wherein the terms “spirit medium” or “curanderismo” were the preferred terms of the practitioners due to their overlapping constructs with shamanism, as described by the authors of those papers. Figure 1 demonstrates the flow of the search and its results. The review was not registered, and no further protocol was prepared.18
Results
Our search produced a total of 124 results. Nine duplicates were removed. Based on a review of the titles and abstracts, of the remaining 115 records, 49 were excluded as irrelevant, 30 for being commentaries, 19 for including psychedelic substances, and 1 which was only available in German. The remaining 16 studies were assessed after retrieval of full-text manuscripts. Ten case reports, two case series described in three publications, and one clinical trial described in three publications are briefly summarized in Table 1.
Table 1: Summary of study findings.
| Citation | Population | Findings |
|---|---|---|
| Case reports | ||
| Woon and Teoh19 | One 27-year-old female in Malaysia | Pt encounters difficult life circumstances including family conflict, being unmarried, and failed attempts to make an independent living. She receives conventional care for depression over the course of a year. For a period of time, she claimed to be possessed by a Goddess of Mercy and intended to follow her path as a spirit medium, a type of shamanic practitioner. The authors point out that traditionally, this spirit inhabited virgin women who were then exempt from marriage for at least 5 years in addition to certain privileges in society. Her circumstances changed, however, and her symptoms improved with conventional care, and she stopped pursuing mediumship. |
| Cramer20 | One 39-year-old male in Mexico | Pt is a community outcast who claims to be a curandero and is possessed by three saints and a doctor. He can elicit the possessions, but they sometimes come on their own. A catholic priest determined that he is not possessed by saints (who do not possess people) or demonic forces. Instead, the author theorizes that while the pt is sincere in his belief that he is possessed, it is a compensatory mechanism for his insecurities. |
| Zethelius and Balick21 | One Colombian male with a poisonous snake bite | A local man presented to the clinic with an infected snake bite on the lower leg. He was treated with antivenom and antibiotics. A shaman also being treated in the clinic also performed a ritual including chanting and blowing of tobacco smoke on him. The ritual calmed the pt’s nerves (lowered heart and respiration rate); however, neither intervention was entirely successful, and the man had to have his lower leg amputated. |
| Tobin and Friedman22 | One 22-year-old male Hmong soldier refugee from Laos living in the United States | Pt experienced nightmares with constricted breathing. A shaman performed a ritual on his behalf, and his immediate symptoms were relieved. He likely experienced PTSD and survivor’s guilt. |
| Etsuko23 | One 43-year-old female with multiple complaints in Japan | The pt described in this case study would likely be diagnosed with schizophrenia or another psychotic disorder. The case describes her evolving view of her illness through her shamanic perspectives. She visits several shamans and attempts their prescriptions; however, even the shamans say “she is strange.” |
| Razali24 | One Malaysian women with conversion disorder | After being told that her husband was taking a second wife, the pt began experiencing paraparesis. Anxiolytics and folk herbal remedies did not improve her condition, but three nights of a shamanic ceremony resulted in expression of emotion and restoration of function in her legs. |
| Hwang et al.25 | One male Filipino immigrant with schizophrenia | Pt believed he was a shaman, which was acceptable in the Philippines, but when he immigrated to the United States, stress and acculturation led to acceptance of mental illness which he considered separate from his shamanic visions. |
| Kennedy et al.26 | One 53-year-old Hispanic male in the Unites States with low back pain | In a primary care setting, this patient was given 33 sessions over 10 months of curanderismo, featuring aromatherapy, massaging of meridians, sound therapy including music and chanting, and spiritual intention setting. Though his pain scores did not decrease significantly, he was able to decrease his use of opioids. |
| Thapa et al.27 | One 47-year male, Nepali shaman | Pt was a shaman who regularly ingested bell clappers (metal rods), which are considered sacred objects, to demonstrate his power. In this case, he ingested four, two of 10 cm length and two of 15 cm, which surprisingly made it to his ileocecal junction, where they ruptured his bowel. They were surgically removed successfully in the ER, and the pt recovered. |
| Rusly et al.28 | One 75-year-old Malaysian woman | Pt had 10 “charm needles” inserted into her face and genitals by a shaman 20 years prior that were discovered on X-ray during evaluation for unrelated complaints. She felt guilty and was preoccupied about having them and was later diagnosed with anxiety. |
| Case series | ||
| Zatzick and Johnson29 | Nine participants of a workshop in urban North America | A single practitioner of “new age” or “alternative healing,” which he termed self-acceptance training, was followed during several workshops. Nine participants consented to reporting of their cases (two of which are reported in greater detail). A variety of methods are discussed and used including Gestalt-oriented therapy, hypnosis, and neo-shamanism (de-possession, dismemberment, etc.). Immediate, 1-month, and 1-year results are reported. Some reported lasting benefit, while others were neutral, though most participants indicated that they had participated or will continue to participate in more workshops even if their results were not significant. |
| Wahbeh et al.30 | Six veterans with PTSD in the United States | A prospective case series collects outcome measures for six veterans going through a neo-shamanic healing intervention. Four completed the series, all of whom saw an improvement in quality of life and three saw a reduction of PTSD symptoms. |
| Clinical trial | ||
| Vuckovic et al.13–15 | 23 women with TMD in the United States | In this phase I feasibility study, 23 women with TMD underwent a protocol of five shamanic practitioner interventions. Qualitative interviews were conducted by non-practitioner investigators. Emergent themes describe physical benefit, enhanced self-awareness, capacity for coping, improved relationships, and self-care practices. Ratings of usual and worst pain, and functional impairment also improved and remained unchanged at 9-month follow-up. |
There was significant diversity in the shamanic practices reported in these studies. Interventions ranged from physical (e.g. needle insertion to ingestion of bell clappers) to the more spiritual (e.g. chanting and ASC). The types of clinical conditions for which patients sought shamanic treatment also varied. These ranged from physical, mental/emotional, to spiritual issues. Only three of these studies were prospective or reported quantitative outcomes. Those three studies reported benefits and no significant harm.14,26,30 However, some of the case reports demonstrated that in some individuals belief in shamanism exposed them to some risks including delayed treatment with conventional care,19,20,23,25,27,28 while others reported a net benefit.21,22,24,29
Discussion
Case Reports
While our original intention was to perform a systematic review, after our search revealed only a single clinical trial, we felt that a broader scope was necessary to capture potential data on the clinical value of shamanic healing; thus, we included case reports in our search. It should come as no surprise that publishing case reports in peer-reviewed medical literature is not a common practice among traditional shamans or Western neo-shamanic practitioners. Furthermore, we excluded commentaries and anthropological literature which may have contained potentially relevant content. Thus, the case reports discussed here should not necessarily be considered representative of shamanic healing as it occurs in practices throughout the world. Although the exact professional background of the authors in most cases is unclear, all 10 studies report their cases from a conventional Western perspective wherein shamanism is part of the cultural context of the case rather than a primary intervention being investigated. Nonetheless, all authors appeared to avoid pathologizing or making disparaging comments about shamanism as a belief system held by the patients who were subjects of the studies.
Interestingly, all 10 of the case reports either take place in countries with deeply ingrained shamanic belief systems or are about immigrants from such cultures. In 6 of the 10 reports, the subject’s belief in shamanism played a significant role in symptomatology as either a causal factor (e.g. Thapa et al.,27 where the subject, believing he had special shamanic powers, swallowed bell clappers which nearly killed him) or a barrier to treatment (e.g. Cramer,20 where the subject claimed shamanic powers to compensate for a disempowered position in society). Three cases (Etsuko,23 Hwang et al.,25 and Thapa et al.27) likely involved schizophrenia. In many traditional shamanic cultures, it is common, if not required, for a shaman to experience some form of healing crisis as an initiation. This can include what would be called a psychotic or manic episode from a Western perspective. The interested reader is encouraged to see Brouwer et al.8 for a thorough discussion on this topic. In these three cases, as well as Cramer20 and Woon and Teoh,19 the subjects were not reported to be highly regarded shamanic healers in their respective communities, but instead were using their cultures’ belief systems to understand and heal their ailments. While these cases resulted in delayed conventional treatment and sometimes harm, there is insufficient evidence to conclude that a shamanic belief system is necessarily dangerous at a cultural level.
There were several reported benefits of the shamanic practices. We previously highlighted the case of Hwang et al.25 for the subject’s belief in shamanism delaying his treatment because of the subject’s initial reluctance to acknowledge his mental illness. However, he reported living with his symptoms reasonably well while living in a rural part of the Philippines where such beliefs are socially acceptable. It was his immigration to the United States where he was unable to maintain stable employment and social relationships that his mental illness and belief system came into conflict. Other benefits included reduced need for pain medication,26 resolution of conversion disorder,24 cessation of nightmares,22 and reduced anxiety.21 While the cases of Tobin and Friedman22 and Kennedy et al.26 included physiological interventions that could contribute to their benefits, such as tobacco smoke easing anxiety and massage reducing the need for pain medication, respectively, belief and ceremony in a culturally contextualized environment likely played a role in the underlying mechanism of benefit.
Case Series
While all the case reports discussed above consisted of shamanism from within cultures that generally accept it, the following case series and clinical trial all take place in the United States with local subjects, where even culturally adapted “neo-shamanic” practices were considered counter-cultural. The first of the two consisted of observations from a series of workshops of a single, unlicensed practitioner reported by Zatzick and Johnson.29 The practitioner blended neo-shamanic practices such as de-possession, dismemberment, and soul retrieval with recognizable Western psychotherapies including Gestalt and hypnosis. There were no diagnoses, inclusion or exclusion criteria, or quantitative measures taken from subjects; however, interviews were conducted, which the authors used to report ethnographic summaries. Many reported at least some benefit from their participation in the workshops; however, at 1 year follow-up, benefits were not consistently maintained. Despite this fact, even those who reported that their benefits had been small and/or short lived said they either had participated or would participate in more workshops, thus indicating that they held their experience in overall positive regard.
The case series by Wahbeh et al.30 was prospective and included quantitative outcome measures. Participants were veterans from prior research studies diagnosed with post-traumatic stress disorder (PTSD). The PTSD Checklist (PCL), the World Health Organization Disability Assessment Schedule 2 (WHODAS 2.0), and the Spiritual Wellness Inventory (SWI) were collected at baseline and after each of eight sessions completed over a 20-week period. Six subjects enrolled, with four completing at least seven sessions.
All four participants saw an improved overall quality of life score as measured by the WHODAS 2.0. Three participants saw a reduction in PTSD symptoms, while the fourth participant saw no change as indicated by PCL scores. The SWI does not provide an aggregate score for overall spiritual wellness, but among its 11 subscales, several improvements were noted including present-centeredness and spiritual freedom. Summaries of each participant’s subjective experience were also reported. The authors report that the subjectively assessed intensity and duration of trauma had the largest impact on variation of outcomes, with those reporting onset of trauma earlier in life and more severe symptoms showing milder improvements. Early positive change from shamanic healing treatments had the largest impact of sustained participation in the intervention. Other factors mentioned included the presence of pre-military trauma, interfering medications, lifestyle behaviors, and home situations. These conclusions, while reasonable, should be considered preliminary due to the small sample size.
Clinical Trial
The only clinical trial that our search revealed was conducted by Vuckovic et al. and published in three reports in 2007,15 2010,13 and 2012.14 It was an uncontrolled, mixed-methods, feasibility study that collected qualitative and quantitative data. The study enrolled 23 women with temporomandibular joint dysfunction (TMD), with 19 completing long-term follow-up. The authors cite evidence that non-responders to allopathic treatment for TMD often have significant psychosocial factors, including depression, that may often correlate with what is called soul loss in the shamanic perspective. After screening, participants were randomized to one of four shamanic practitioners for a series of five treatments. A study investigator then conducted interviews at 1, 3, 6, and 9 months post-treatment to assess usual pain, worst pain, and functional impairment using an 11-point Likert scale and collected qualitative data.
Results at study completion showed a statistically significant decline in usual pain, worst pain, and functional impairment.15 Long-term follow-up showed no significant changes from results at completion, indicating that effects were stable at least 9 months post-treatment.14 From qualitative interviews completed at follow-up (n=19), the authors applied a matrix coding process to the two main themes of change in TMD symptoms and reported changes in psychosocial well-being. This resulted in categorizing participants into five types as follows: “no TMD symptoms and consistent positive changes in psychosocial well-being” (n=3), “TMD symptoms still perceptible but improved, and consistent positive changes in psychosocial well-being” (n=11), “reduced TMD pain, but inconsistent or missing reports on psychosocial changes” (n=2), “TMD very painful since ending treatment, but consistent positive changes in psychosocial well-being” (n=1), and “increasing TMD pain and minimal positive changes in psychosocial well-being” (n=2). The authors state that despite the study’s limitations, it demonstrates the feasibility of investigating shamanic healing as an intervention, and while not conclusive, it was effective in reducing pain in women with TMD, warranting further research.
Limitations
While there is an abundance of literature on shamanism as a spiritual practice, most of that literature resides in the discipline of anthropology. As health science researchers, the authors decided to limit the scope of the present review to peer-reviewed medical literature of shamanic healing while excluding the use of psychedelic substances. While the inclusion of case reports added insight into the cross-cultural practices of shamanic healing, their heterogeneity in population and methods and lack of quantitative data make it challenging to draw conclusions from them. Furthermore, the case series and one feasibility study discussed here lacked control groups, collection of data on expectancy or prior beliefs, and large enough cohorts to power strong statistical analysis. In light of these limitations, our results should be considered preliminary.
Conclusion
A recurring theme in the case reports was an emphasis on the need for a culturally appropriate approach to providing clinical care. This is as true for patients coming from cultures with shamanic belief systems as for those with any other spiritual or religious belief system such as those in Western settings. Future research in shamanic healing would benefit from collecting data on expectancy and belief to determine the role of belief in clinical outcomes. Nonetheless, the two case series and the clinical trial demonstrated the feasibility of shamanic healing as an intervention with a low risk of harm and some potential benefits, at least in the case of PTSD and TMD. Further research is warranted to investigate the potential value of shamanic healing as a clinical intervention.
Competing Interests
The authors declare they have no competing interests.
Authors' Contributions
Both MRH and REH contributed to the conceptualization. MRH was responsible for writing the original draft, methodology, and formal analysis. REH was responsible for reviewing and editing the writing and supervision. All authors read and approved the final manuscript.
Acknowledgements and Funding
MRH was funded by NIH-NCCIH T32 AT002688.
References
- Singh M. The cultural evolution of shamanism. Behav Brain Sci. 2017;41:e66.
- Winkelman MJ. The evolved psychology of psychedelic set and setting: inferences regarding the roles of shamanism and entheogenic ecopsychology. Front Pharmacol. 2021;12:619890.
- Şenel E. Health and ancient beliefs: a scientometric analysis of health literature related to shamanism, paganism and spirituality. J Relig Health. 2019;58(6):2019–35.
- Eliade M. Shamanism: Archaic Techniques of Ecstasy. Princeton: Princeton University Press; 1964.
- Harner M. The Way of the Shaman. Harper Collins; 1980.
- Scuro J, Rodd R. Neo-Shamanism. In: Gooren HPP, ed. Encyclopedia of Latin American Religions. Cham: Springer International Publishing; 2014. pp. 1–6.
- Walsh R, Grob CS. Higher Wisdom: Eminent Elders Explore the Continuing Impact of Psychedelics. State University of New York Press; 2005.
- Brouwer A, Winkelman MJ, Raison CL. Shamanism: psychopathology and psychotherapy. Religion Brain Behav. 2025;15:26–43.
- Dobkin de Rios M, Winkelman M. Shamanism and altered states of consciousness: an introduction. J Psychoactive Drugs. 1989;21(1):1–7.
- Neher A. Auditory driving observed with scalp electrodes in normal subjects. Electroencephalogr Clin Neurophysiol. 1961;13:449–51.
- Neher A. A physiological explanation of unusual behavior in ceremonies involving drums. Hum Biol. 1962;34:151–60.
- Huels ER, Kim H, Lee U, et al. Neural correlates of the shamanic state of consciousness. Front Hum Neurosci. 2021;15:610466.
- Vuckovic NH, Schneider J, Williams LA, Ramirez M. Journey into healing: the transformative experience of shamanic healing on women with temporomandibular joint disorders. Explore. 2010;6(6):371–9.
- Vuckovic NH, Williams LA, Schneider J, et al. Long-term outcomes of shamanic treatment for temporomandibular joint disorders. Perm J. 2012;16(2):28–35.
- Vuckovic NH, Gullion CM, Williams LA, et al. Feasibility and short-term outcomes of a shamanic treatment for temporomandibular joint disorders. Altern Ther Health Med. 2007;13(6):18–29.
- Dos Santos FC, Macieira TGR, Yao Y, et al. The impact of spiritual care delivered by nurses on patients’ comfort: a propensity score matched cohort utilizing electronic health record data. Int J Med Inform. 2023;183:105319.
- De Diego Cordero R, Velasco-Domínguez C, Aranda-Jerez A, Vega-Escaño J. The spiritual aspect of pain: an integrative review. J Relig Health. 2024;63(1):159–84. https://doi.org/10.1007/s10943-023-01890-9.
- Haddaway NR, Page MJ, Pritchard CC, McGuinness LA. PRISMA2020: an R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell Syst Rev. 2022;18(2):e1230.
- Woon TH, Teoh CL. Psychotherapeutic management of a potential spirit medium. Aust N Z J Psychiatry. 1976;10(1A):125–8.
- Cramer M. Psychopathology and shamanism in rural Mexico: a case study of spirit possession. Br J Med Psychol. 1980;53(1):67–73.
- Zethelius M, Balick MJ. Modern medicine and shamanistic ritual: a case of positive synergistic response in the treatment of a snakebite. J Ethnopharmacol. 1982;5(2):181–5.
- Tobin JJ, Friedman J. Spirits, shamans, and nightmare death: survivor stress in a Hmong refugee. Am J Orthopsychiatry. 1983;53(3):439–48.
- Etsuko M. The interpretation of fox possession: illness as metaphor. Cult Med Psychiatry. 1991;15:453–77.
- Razali SM. Conversion disorder: a case report of treatment with the Main Puteri, a Malay shamanastic healing ceremony. Eur Psychiatry. 1999;14(8):470–2.
- Hwang WC, Miranda J, Chung C. Psychosis and shamanism in a Filipino-American immigrant: clinical case study. Cult Med Psychiatry. 2007;31(2):251–69.
- Kennedy L, Gonzales E, Corbin L. The effect of curanderismo on chronic non-malignant pain: a case report. Explore. 2016;12(4):263–7.
- Thapa N, Basnyat S, Maharjan M. Ingestion of bell clappers by a Shaman in Jumla, Nepal: a case report. JNMA J Nepal Med Assoc. 2019;57(215):56–8.
- Rusly MFR, Md Yasin M, Kamaruddin KN, et al. The Agony of the Mystical Practice of Susuk: A Case Report. Am J Case Rep. 2022;23: e937633.
- Zatzick DF, Johnson FA. Alternative psychotherapeutic practice among middle class Americans: I: case studies and follow-up. Cult Med Psychiatry. 1997;21(1):53–88.
- Wahbeh H, Shainsky L, Weaver A, Engels-Smith J. Shamanic healing for veterans with PTSD: a case series. Explore. 2017;13(3):207–17.